
接上文Part.1
Second-line Migraine Preventive Therapy/二线偏头痛预防疗法
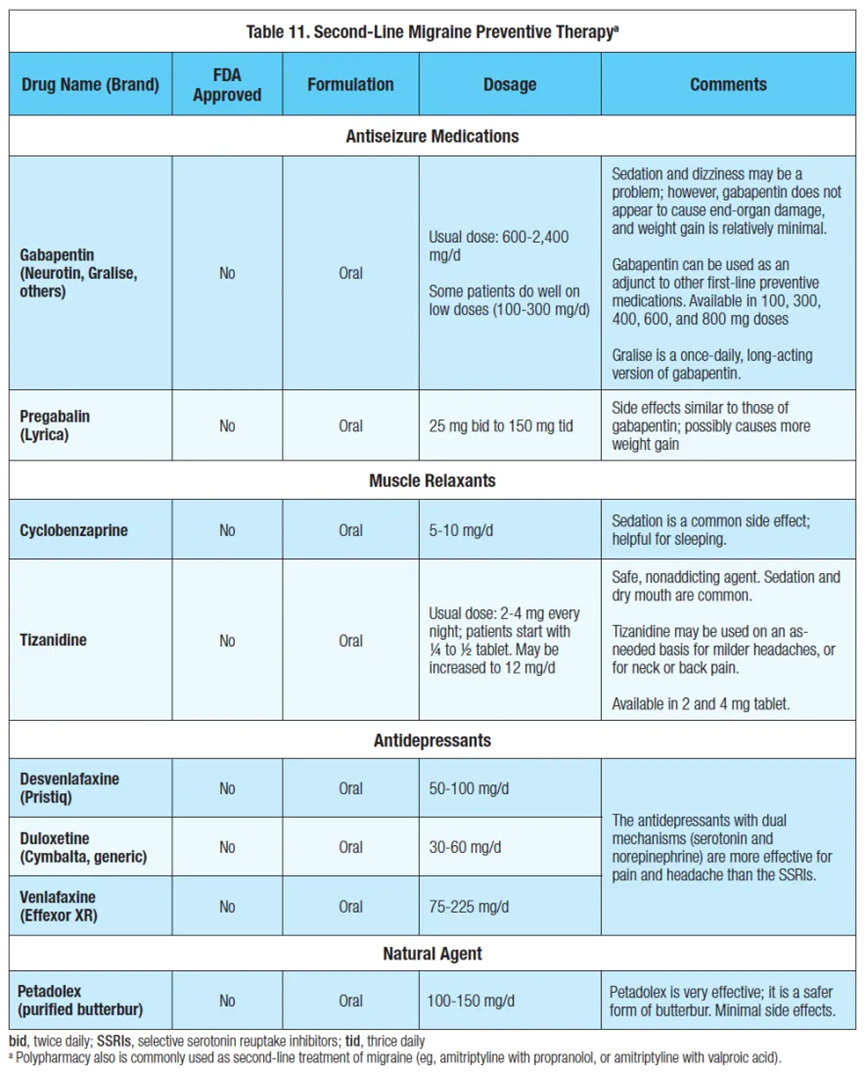
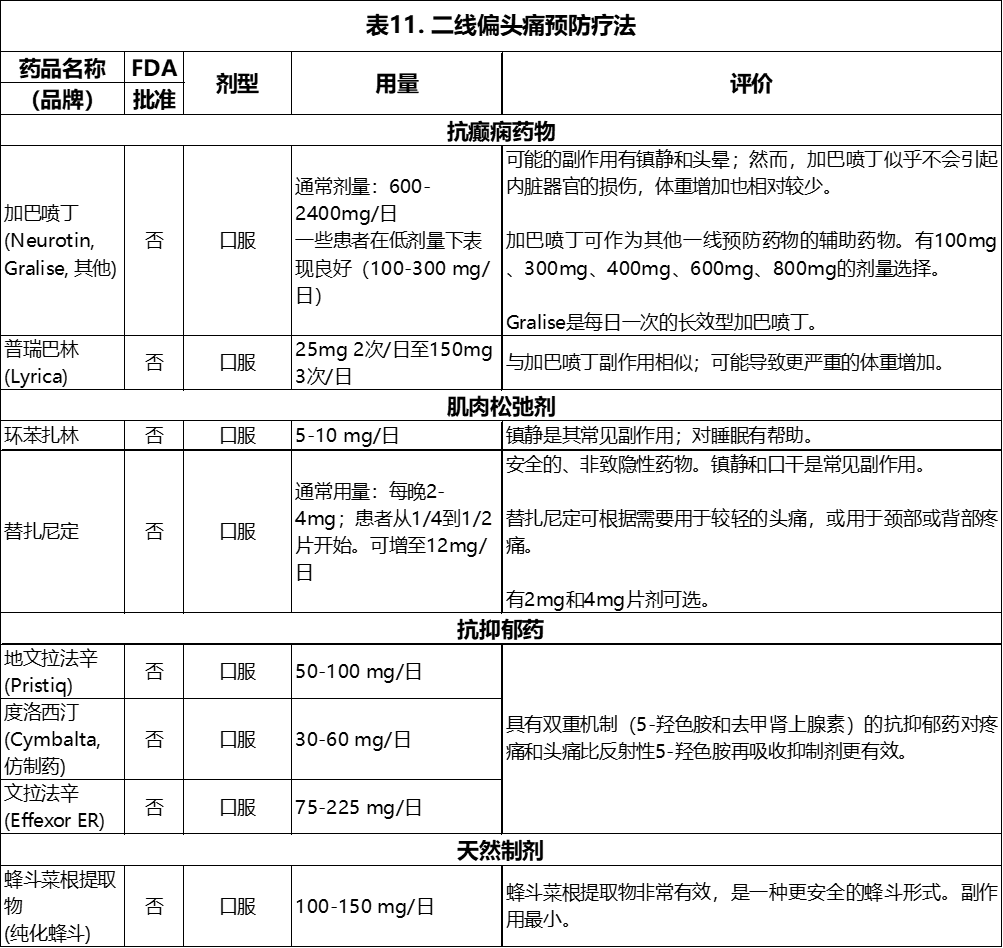
There are a number of second-line migraine treatments. The anti-seizure medication gabapentin has been demonstrated to be mildly useful in migraine and tension headache prophylaxis. In a large study on migraine, doses averaged approximately 2,400 mg per day, but lower doses are usually prescribed.⁵ Some patients do well with very low doses (200 or 300 mg per day). Sedation and dizziness may be a problem; however, gabapentin does not appear to cause end-organ damage, and weight gain is relatively minimal. Gabapentin can be used as an adjunct to other first-line preventive medications. Pregabalin (Lyrica) has a similar mechanism of action to gabapentin. Lyrica is fairly safe, but sedation and weight gain often occur.
偏头痛的二线治疗方法有很多。抗癫痫药物加巴喷丁已被证明对偏头痛和紧张性头痛的预防有轻微作用。在一项关于偏头痛的大型研究中,平均剂量约为每天2,400mg,但通常处方剂量较低。⁵有些病人用很低的剂量(每天200或300mg)就能取得很好的疗效。镇静和头晕是可能的副作用;但是,加巴喷丁似乎不会引起终末器官损伤,而且体重增加相对较少。加巴喷丁可作为其他一线预防药物的辅助药物。普瑞巴林(Lyrica)的作用机制与加巴喷丁相似。Lyrica是相当安全的,但经常会出现镇静作用和体重增加。
A safe, non-addicting muscle relaxant, tizanidine is useful for migraine and chronic daily headache. Tizanidine may be used on an as-needed basis for milder headaches, or for neck or back pain. Cyclobenzaprine (10 mg) is helpful for sleeping, and helps some with migraine and chronic daily headache.
替扎尼定是一种安全、非成瘾性的肌肉松弛剂,对偏头痛和慢性日常头痛有用。替扎尼定可根据需要用于轻度头痛,或颈部或背部疼痛。环苯扎林(10mg)有助于睡眠,并对一些偏头痛和慢性日常头痛有帮助。
There have been a number of studies on the efficacy of using angiotensin receptor blockers (ARBs) and the angiotensin-converting enzyme inhibitors (ACEs) for the prevention of migraine. ARBs are preferred because of minimal side effects. Examples include losartan (Cozaar) and candesartan (Atacand). These may be useful for the patient with hypertension and migraine. Side effects include dizziness, among others, but they are usually well tolerated, with no sedation or weight gain.
关于使用血管紧张素受体阻断剂(ARBs)和血管紧张素转换酶抑制剂(ACEs)预防偏头痛的功效,已经有许多研究。ARBs是首选,因为其副作用最小。例如洛沙坦(Cozaar)和坎地沙坦(Atacand)。这些药物可能对高血压和偏头痛患者有用。副作用包括头晕等,但通常耐受性良好,不会产生镇静作用或体重增加。
Similar to the ARBs, the calcium channel antagonists have been utilized for migraine prevention. Verapamil ER (extended release) is the most commonly used form, with doses ranging from 120 mg daily up to 360 mg per day. Verapamil is probably more effective as a cluster headache preventive.
与ARBs类似,钙离子通道拮抗剂也被用于预防偏头痛。维拉帕米ER(缓释)是最常用的形式,剂量从每天120mg到每天360mg不等。维拉帕米作为丛集性头痛的预防类药剂可能更有效。
Polypharmacy is common in migraine prevention. Two first-line medications often are used together, and the combination of 2 preventives can be more effective than a single drug alone. For example, valproate often is combined with an antidepressant. Amitriptyline may be combined with propranolol (or other β-blockers), particularly if the tachycardia of the amitriptyline needs to be offset by a β-blocker; this combination is commonly used for “mixed” headaches (migraine plus chronic daily headache.) NSAIDs may be combined with most of the other first-line preventive medications. Thus, naproxen often is given with amitriptyline, propranolol, or verapamil. Naproxen is employed simultaneously as preventive and abortive medication. Polypharmacy commonly is employed when significant comorbidities (anxiety, depression, hypertension, etc.) are present. Unfortunately, polypharmacy brings the risk of increased side effects.
多药联用在偏头痛预防中很常见。两种一线药物通常一起使用,2种预防药物的组合可能比单独使用一种药物更有效。例如,丙戊酸钠常与一种抗抑郁药联合使用。阿米替林可与普萘洛尔(或其他β-受体阻滞剂)联合使用,特别是当阿米替林的副作用心动过速需要被β-受体阻滞剂抵消时;这种组合通常用于 "混合型 "头痛(偏头痛加慢性日常头痛)。非甾体抗炎药可与大多数其他一线预防药物联合使用。因此,萘普生经常与阿米替林、普萘洛尔或维拉帕米一起服用。萘普生可同时作为预防剂和中止剂使用。当存在严重的合并症(焦虑、抑郁、高血压等)时,通常采用多种药物治疗。不幸的是,使用多种药物会带来副作用增加的风险。
Venlafaxine (Effexor XR) is an excellent antidepressant, occasionally helpful for the prevention of migraine. It is used primarily as an SSRI at lower doses; at higher doses (100-150 mg) norepinephrine also is increased. In fact, antidepressants with dual mechanisms (serotonin and norepinephrine) are more effective for pain and headache. Another similar medication is duloxetine (Cymbalta), with typical doses being 30 mg to 60 mg daily. Cymbalta has several pain indications, but is probably more effective for moods than for headache.
文拉法辛(Effexor XR)是一种很好的抗抑郁药,偶尔也有助于预防偏头痛。它在低剂量时主要作为SSRI使用;在高剂量时(100-150mg)去甲肾上腺素也会增加。事实上,具有双重机制(5-羟色胺和去甲肾上腺素)的抗抑郁药对疼痛和头痛更有效。另一种类似的药物是度洛西汀(Cymbalta),典型剂量为每天30mg至60mg。Cymbalta有几个疼痛适应症,但对情绪的治疗可能比对头痛的治疗更有效。
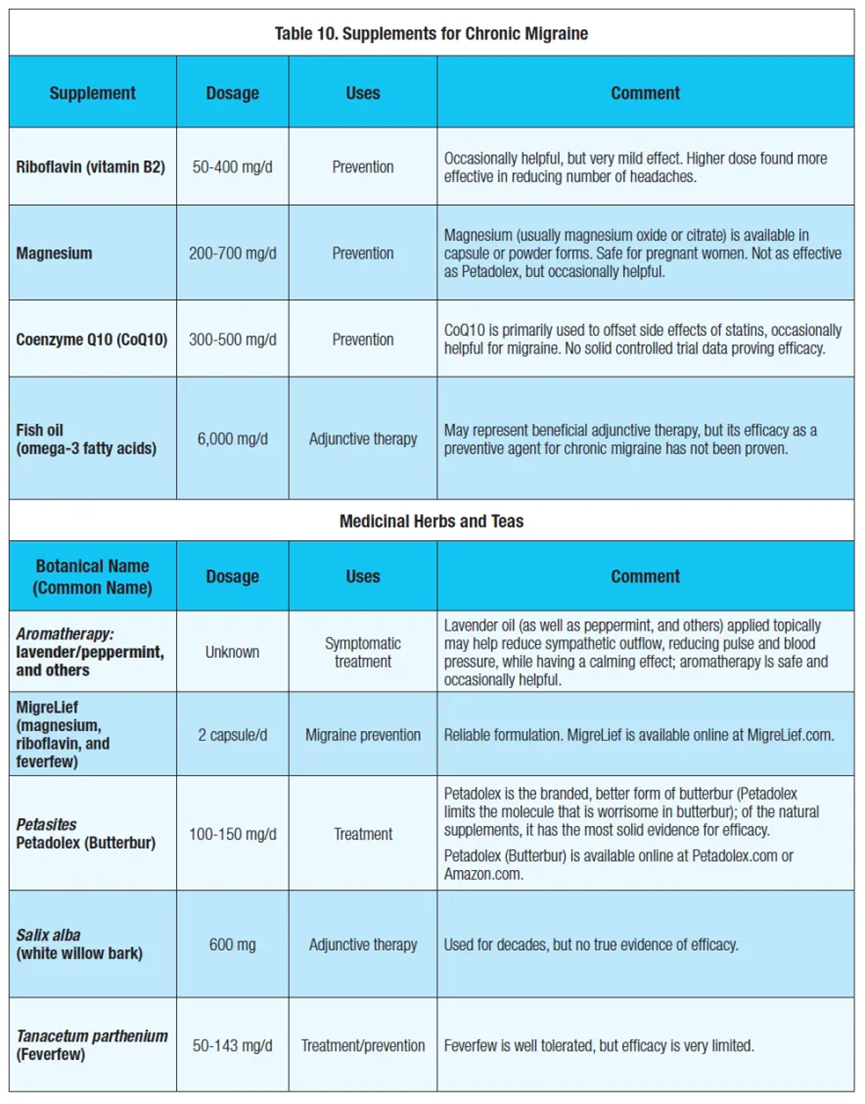
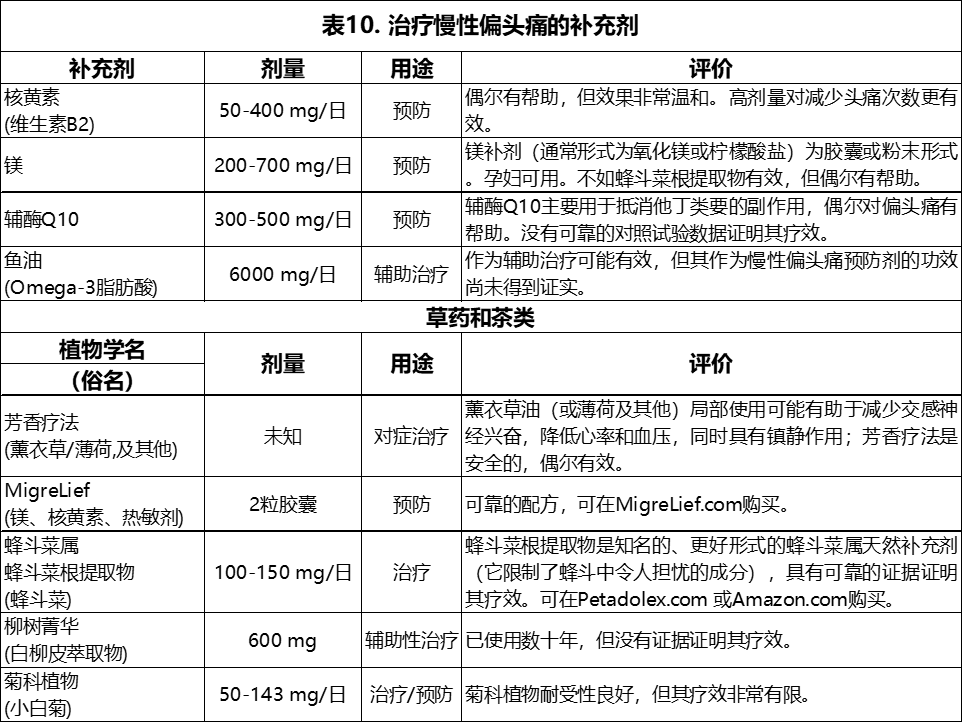
A review of second-line treatment can be found in Table 10.⁶
关于二线治疗的综述见表10.⁶
What's New in Headache/关于头痛治疗的最新进展
Transcranial magnetic stimulation (TMS) has been the primary new therapy to emerge. In addition to TMS, ketamine is (occasionally) being utilized for refractory headaches. Calcitonin gene-related peptide (CGRP) inhibitors are in the late stages of development for the prevention of migraine; however, if they are approved, CGRP inhibitors will not be available until mid-2018 (at the earliest).
经颅磁刺激(TMS)已成为主要的新疗法出现。除TMS外,氯胺酮(偶尔)也被用于治疗难治性头痛。降钙素基因相关肽(CGRP)抑制剂正处于预防偏头痛的后期开发阶段;然而,即使获得批准,CGRP抑制剂将在2018年中(最早)才能上市。
Transcranial Magnetic Stimulation(TMS)/经颅磁刺激(TMS)
TMS has primarily been utilized for depression. The repetitive TMS units give thousands of pulses in an hour. The SpringTMS (from eNeura) hand-held system imparts only a single pulse. There have been a number of well-done studies on TMS for headache and depression. The patient uses a hand-heldTMS device, 4 pulses twice daily (as a preventive). This takes about 5 to 10 minutes for the 4 pulses. TMS may be used abortively as well. Long-term efficacy is not well established. However, early results are promising, at least for a subset of refractory chronic migraineurs. TMS has been safe, although some patients do not like the “thump” that each pulse imparts. The cost is $450 for the first 3 months (the company rents the machine to the user).
TMS主要用于治疗抑郁症。重复的TMS装置每小时能发出数千次脉冲。SpringTMS(来自eNeura)手持式系统只提供单个脉冲。有许多关于TMS治疗头痛和抑郁症的研究已经完成。病人使用手持式TMS设备,每天4次脉冲(作为预防手段)。这4次脉冲大约需要5至10分钟。TMS也可用于中止性治疗。长期疗效尚不明确。然而,早期的结果是很有希望,至少对一部分难治性慢性偏头痛患者来说是如此。TMS是安全的,尽管有些病人不喜欢每个脉冲带来的 "砰 "的一声。前三个月的费用是450美元(公司向用户出租机器)。
Ketamine/氯胺酮
Ketamine has been used to treat refractory pain or depression for the past several years. Ketamine is an NMDA receptor glutamate antagonist. In addition, ketamine affects several other receptors as well. Ketamine has been used for treatment-resistant depression, primarily as the IV formulation. Ketamine has been a drug of abuse, and has major addiction potential. There have been a number of successful trials utilizing ketamine, either intravenously or as a nasal spray. A nasal spray form of Ketamine may be marketed for severe depression in 2019.
氯胺酮在过去几年中一直用于治疗难治性疼痛或抑郁症。氯胺酮是一种NMDA受体谷氨酸拮抗剂。此外,氯胺酮也会影响其他几种受体。氯胺酮已被用于治疗难治性抑郁症,主要作为静脉制剂。氯胺酮一直是一种滥用药物,具有很大的成瘾可能性。已经有一些利用氯胺酮的成功试验,无论是静脉注射还是鼻腔喷雾。氯胺酮的鼻喷雾剂可能会在2019年上市,用于治疗严重抑郁症。
Theintravenous treatment may be more effective than using ketamine as a nasal spray. However, this author has found that the nasal spray is exceedingly well tolerated, with few side effects. The usual side effects include feeling euphoric, sleepy, dizzy, and (with the IV form) hallucinations.
使用静脉注射治疗可能比使用氯胺酮鼻腔喷雾剂更有效。然而,笔者发现鼻喷雾剂的耐受性非常好,几乎没有副作用。通常的副作用包括感觉愉快、困倦、头晕和(静脉注射形式)幻觉。
This author has utilized ketamine for 42 refractory headache patients, some of whom also suffered from severe depression. Our results indicated that ketamine is more helpful for the depression than the pain. The decrease in headache tends to be short-lived. However, certain patients do well with both depression and headache. We have used only the nasal spray. It is formulated as a liquid, 10 mg ketamine per 0.1 mL. The patient does the treatment in our office once per week. The usual dose is 10 mg (one spray) every 10 to 15 minutes. Usually, the total dose for the treatment ranges from 50 mg to 100 mg. We check vitals after every 2 sprays (occasionally blood pressure will rise with ketamine).
笔者曾利用氯胺酮治疗42名难治性头痛患者,其中一些患者还患有严重的抑郁症。结果表明,氯胺酮对抑郁症的帮助比对疼痛的帮助更大。头痛的减少通常是短暂的。然而,某些病人对抑郁症和头痛方面都表现良好。我们只使用了鼻腔喷雾剂。它的配方是液体,每0.1ml含10mg氯胺酮。病人每周在我们的办公室做一次治疗。通常的剂量是每10至15分钟10mg(一喷)。通常,治疗的总剂量在50mg到100mg之间。每喷2次后我们会检查生命体征(氯胺酮偶尔会使血压升高)。
New Formulations/新配方
Several newer formulations of older migraine medications have emerged. Onzetra nasal powder is a new form of sumatriptan nasal spray. Onzetra uses a unique “breath powered” delivery system. Onzetra delivers 11 mg of sumatriptan powder per breath; the usual dose is 22 mg at one time. This places the sumatriptan powder posteriorly, where there is respiratory epithelium. This epithelium is more conducive for absorption of medication than is the anterior squamous epithelium. Onzetra has excellent efficacy, and is well tolerated.
几种老式偏头痛药物的新配方已经出现。Onzetra鼻粉是一种新形式的舒马曲坦鼻喷雾剂。Onzetra采用了一种独特的 "呼吸动力 "给药系统。Onzetra每次呼吸提供11mg苏马曲坦粉末;通常的剂量是一次服用22mg。这样的方式会将苏马曲坦粉末放在呼吸道上皮的后部。这种上皮细胞比前部鳞状上皮细胞更有利于药物的吸收。Onzetra有很好的疗效,而且耐受性良好。
Trokendi XR is a long-acting formulation of topiramate. Trokendi has the indication for migraine prophylaxis. In our (anecdotal) experience, approximately 70% of patients prefer the Trokendi XR, versus the generic topiramate.
Trokendi XR是托吡酯的一种长效制剂。Trokendi的适应症是预防偏头痛。根据我们的(传闻)经验,大约70%的病人偏向使用Trokendi XR,多过一般的托吡酯。
Medical cannabis has been used for about 5,000 years. Cannabis has multiple active ingredients—tetrahydrocannabinol (THC) is the main cannabinoid for analgesia and also produces the euphoric effect. Cannabidiol (CBD), the other important compound, is an anti-inflammatory. CBD also may enhance analgesia. One advantage of medical marijuana is that the dispensary is able to manipulate the percentage of THC vs. CBD. It often takes weeks to months in order to achieve optimum results. Vaporized inhalation is the most commonly employed route. Marijuana may help with anxiety as well as the pain.
医用大麻的使用已有约5000年的历史。大麻具有多种活性成分 - 四氢大麻酚(THC)是主要的镇痛类大麻素,也产生欣快作用。大麻二酚(CBD)是另一种重要的化合物,是一种抗炎剂。CBD还可以增强镇痛作用。医用大麻的一个优点是药房能够操纵THC与CBD的百分比。通常需要数周至数月才能达到最佳效果。汽化吸入是最常用的方法。大麻可有助于缓解焦虑和疼痛。
Vagal Nerve Stimulation/迷走神经刺激疗法
Non-invasive vagal nerve stimulation (VNS)—the gammaCore VNS system from the company electroCore— was approved in April 2017 for use in episodic cluster headache (not yet approved for migraine) in adults. VNS may suppress glutamate levels in the trigeminal nucleus caudalis, resulting in decreased head pain. The portable gammaCore VNS has demonstrated efficacy for cluster headache. The long-term results in migraineurs has yet to be established. This form of VNS has minimal side effects or dose limitations. The device is not indicated for patients with an active implantable medical device, such as a pacemaker or hearing aid; those with carotid atherosclerosis, or who have had a cervical vagotomy. Also patients with hyper- or hypotension, bradycardia, or tachycardia are not candidates for the device.
非侵入性迷走神经刺激(VNS)--来自electroCore公司的gammaCore VNS系统--于2017年4月被批准用于成人发作性丛集性头痛(尚未批准用于治疗偏头痛)。VNS可抑制三叉神经尾状核中的谷氨酸水平,从而减轻头部疼痛。便携式gammaCore VNS已证实对丛集性头痛有疗效。对偏头痛患者的长期疗效尚未确定。这种形式的VNS的副作用或剂量限制都很小。该设备不适用于佩戴有源植入式医疗设备的患者,如心脏起搏器或助听器;以及颈动脉粥样硬化的患者,或做过颈部迷走神经切断术的患者也不适用。另外,患有高血压或低血压、心动过缓或心动过速的患者也不适合使用该设备。
Conclusion/结论
Migraine is a common and disabling illness. Outside of meds, it is important for migraineurs to watch their headache triggers, and exercise regularly. Physical therapy and/or psychotherapy may be of help (“it takes a village”). There is no good algorithm for determining which medication is best. Each patient is unique, and comorbidities drive where we go with treatment. The goal is to decrease head pain, while minimizing medications.
偏头痛是一种常见的致残性疾病。除药物治疗外,偏头痛患者还必须注意他们的头痛诱因,并定期锻炼。物理治疗和/或心理治疗可能会有帮助("这需要一个村庄的力量")。没有一个很好的公式来确定用哪种药物治疗效果最好。每个病人都是独一无二的,对合并症的考量决定了治疗方向。治疗的目标是减少头部疼痛,同时尽量减少用药。
REFERENCES/参考文献
1. Lipton RB. Bigal ME, Diamond M, et al. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. 2007;68(5):342-349.
2. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders. 2nd ed. Oxford, England: Blackwell Publishing; 2003.
3. Gardner KL. Genetics of migraine: an update. Headache. 2006;46 Suppl 1:S19-S24.
4. Lipton RB, Varon SF, Grosberg B, et al. OnabotulinumtoxinA improves quality of life and reduces impact of chronic migraine. Neurology. 2011;77(15):1465-1472.
5. Mathew NT, Rapoport A, Saper J, et al. Efficacy of gabapentin in migraine prophylaxis. Headache. 2001;41(2):119-128.
6. Robbins Headache Clinic. Robbins Headache Clinic. Available at: www.chicagoheadacheclinic.com. Accessed May 18, 2017.
Notes: This article was originally published June 15, 2017 and most recently updated March 5, 2019. MIGRAINE Volume17, Issue5.

本公众号发布内容未经书面允许不得擅自转载及使用
公众号、报刊转载请联系授权:yannayin@fmchina.org
商务合作请联系:hugh@fmchina.org
欲了解更多:http://fmchina.org
相关信息请登录:http://edu.idhealth.cn/
- 还没有人评论,欢迎说说您的想法!