
译者:李昭兴
接上文
Miscellaneous Approaches/其他方法
Muscle relaxants (carisoprodol, diazepam) or tranquilizers (clonazepam, alprazolam) occasionally are useful, primarily to aid in sleeping. Intravenous sodium valproate (Depacon) is safe and can be effective. The atypical antipsychotics, such as olanzapine (Zyprexa) or quetiapine (Seroquel), occasionally may be useful on an as-needed basis. In the emergency room, IV administration of antiemetic agents such as prochlorperazine (Compazine, others) or metoclopramide (Reglan) may be useful.
肌肉松弛剂(carisoprodol, diazepam)或镇静剂(clonazepam, alprazolam)偶尔是有用的,主要用于帮助睡眠。静脉注射丙戊酸钠(Depacon)是安全有效的。非典型抗精神病药物,如奥氮平(Zyprexa)或喹硫平(Seroquel),在根据需要的情况下使用可能有效。在急诊室里,静脉注射止吐剂如丙氯拉嗪(Compazine,其他)或甲氧氯普胺(Reglan)也可能有帮助。
Certain preventive medications, such as valproic acid (Depakote), topiramate (Topamax), and amitriptyline, may be useful on an as-needed basis, utilizing low doses every 4 to 6 hours. The antihistamine diphenhydramine is occasionally useful when administered intramuscularly. At times, patients may have injections for home use: ketorolac, orphenadrine, sumatriptan, diphenhydramine, promethazine, etc.
某些预防性药物,如丙戊酸(双丙戊酸)、托吡酯(Topamax)和阿米替林,根据需要每4至6小时使用低剂量可能有效。抗组胺药苯海拉明在肌肉注射时也偶尔有效。有时,患者可以在家使用注射剂:酮咯酸、奥非那君、舒马曲坦、苯海拉明、异丙嗪等。
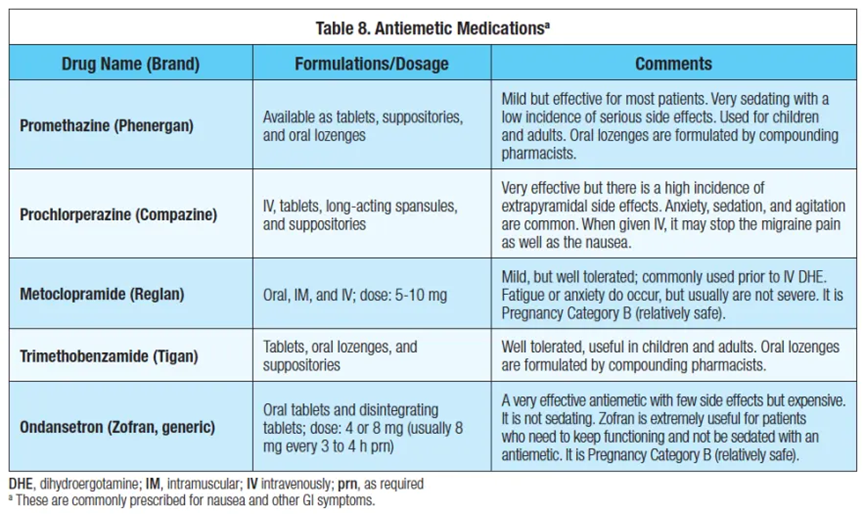
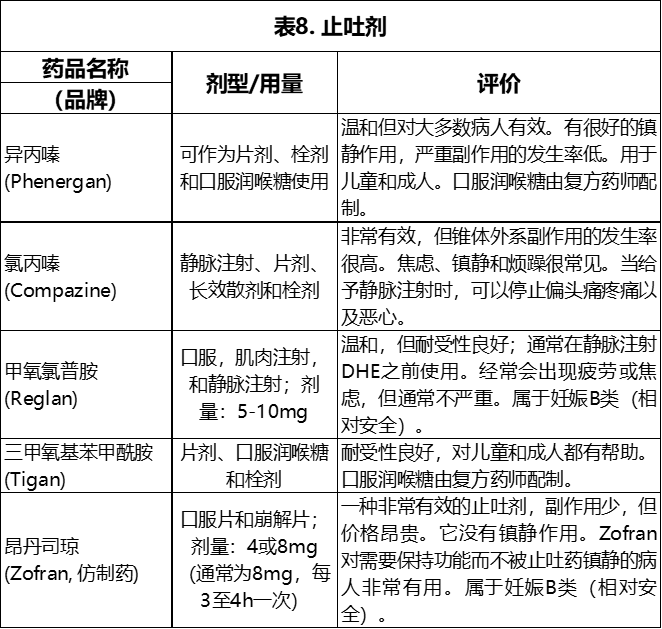
Antiemetic Medications/止吐剂
Table 8 outlines commonly prescribed antiemetic agents for the management of nausea and other gastrointestinal (GI) symptoms.
表8列出了用于治疗恶心和其他消化道(GI)症状的常用止吐剂。
Medication Overuse Headache (MOH)/用药过度的头痛(MOH)
Much is written about MOH, with many patients diagnosed with this condition. Often a patient will be overusing abortive medications (medication overuse), but not be suffering “rebound/withdrawal” headaches (medication overuse, but NOT medication overuse headache). Up until recently, all NSAIDS were lumped under “meds that cause MOH,” and this simply is not true. For some patients, opioids, butalbital, and high-caffeine containing meds cause MOH. Triptans are occasionally implicated as well. However, for most patients with chronic migraine, they have daily (or near-daily) headaches, the preventives may not be effective, and they use abortives in an attempt to get through the day.
已有很多关于MOH的文章讲述许多患者被诊断患有这种疾病。通常病人会过度使用中止性药物(药物过度使用),而不会遭受“反弹/戒断”头痛(有用药过度的情况,但不是用药过度造成的的头痛)。直到最近,所有的非甾体抗炎药都被归为“导致MOH的药物”,这是不正确的。对一些患者来说,阿片类药物、布他比妥和高咖啡因含量的药物都会导致MOH。曲坦类药物偶尔也牵涉其中。然而,对于大多数慢性偏头痛患者来说,每天(或几乎每天)都遭受头痛,一些预防类药剂可能并不有效,他们试图用中止剂来度过这一天。
There are more questions in the area of MOH than we have answers. The pathophysiology of MOH is unclear. Some patients will have MOH from 2 Excedrin daily, while others do not suffer from MOH consuming 8 per day. When patients are using frequent abortives, we often withdraw them from that abortive, push preventives, and attempt to minimize analgesics. However, for many chronic migraine sufferers, the preventives are not very effective. For those sufferers, abortives allow them to live with a reasonable quality of life.
在MOH领域的问题比我们的答案还要多。MOH的病理生理学尚不清楚。有些病人每天吃两片Excedrin就会出现MOH,而有些病人每天吃8片都不会出现MOH。当病人频繁使用中止剂时,我们通常会让病人退出该中止剂,采取预防类药剂,并尽量减少镇痛剂的使用。然而,对于许多慢性偏头痛患者来说,预防类药剂并不十分有效。对于这些患者来说,中止剂使他们能够以更合理的生活质量生活。
Preventive Medications/预防性药物
There is no algorithm to determine who is to go on preventive headache medication. The number of monthly headaches is one factor, along with comorbidities. Patients have to be willing to take daily medication (many do not want any daily meds). There is no absolute rule that applies to headache treatment. For a patient with two headaches a month that are severe, prolonged, and not relieved by drugs, preventive medicine might be used. On the other hand, for the person who has five headaches a month, but can obtain relief from Excedrin or a triptan, preventive medicine may not be optimal. The choice of who qualifies for medication depends on the patient’s age, medical and psychiatric comorbidities, and frequency and severity of the migraine, as well as the patient’s preference. Comorbidities often determine which preventive meds are used. If a patient has HTN, a med for blood pressure will be used. When patients concurrently suffer with anxiety or depression, various antidepressants are utilized for the headache and mood disorder. We want to minimize meds, and treating 2 conditions with one medication is ideal.
目前还没有公式来判断哪些人能够接受预防性头痛药物治疗。每月头痛的次数及合并症是一个因素。患者必须愿意每天服药(许多人不希望有任何日常用药)。没有适用于头痛治疗的绝对公式。对于一个月有两次严重的、长时间的、药物不能缓解的头痛病人,可能会使用预防类药剂。另一方面,对于一个月有五次头痛,但可以通过Excedrin或曲坦类药物获得缓解的人来说,预防类药剂可能不是最佳选择。选择符合用药条件的人取决于病人的年龄、医疗和精神方面的合并症、偏头痛的频率和严重程度,以及病人的偏好。合并症往往决定使用哪种预防类药剂。如果病人有高血压,可以使用治疗血压的药物。如果病人同时患有焦虑症或抑郁症,就可以使用各种抗抑郁药来治疗头痛和情绪紊乱。我们希望尽量减少用药,用一种药物治疗两种疾病是最理想的情况。
In using medication, a realistic goal is to decrease the headache severity by 40% to 70%, not to completely eliminate the headaches. It is wonderful when the headaches are 90% improved, but the idea is also to minimize medication. “Clinical meaningful pain relief” is usually around a 30% improvement. Most patients need to be willing to settle for moderate improvement. Preventives may take 3 to 6 weeks to work, and “educated guesswork” often is used to find the best approach for each patient. In the long run, preventive medications are effective for approximately 50% of patients. The other 50% scramble with various abortives.
在使用药物时,一个现实的目标是将头痛的严重程度降低40%到70%,而不是完全消除头痛。头痛得到90%的缓解是件好事,但同时也要尽量减少药物治疗。"临床意义上的疼痛缓解"通常是大约30%的改善。大多数病人需要愿意接受适度的改善。预防类药剂可能需要3到6周的时间才能发挥作用,并经常使用“临床经验推论”用来为每个患者找到最佳的治疗方法。从长远来看,预防类药剂治疗对大约50%的患者有效。另外50%的人使用中止性药物抗击头痛。
As noted, patients should play an active role in medication choice. Preventive medications should be selected depending on the patient’s medical and psychological comorbidities, GI system, medication sensitivities, weight, sleep, family history of reaction to medications, finances, willingness to take daily meds, and many other factors. Fatigue and/or weight gain are major reasons why patients abandon a preventive medication. Headache patients commonly complain of fatigue, and tend to give up on medications that increase tiredness. A patient’s occupation also may guide the caregiver away from certain medications; for example, an accountant may not be able to tolerate the memory problems associated with topiramate.
如前所述,患者本身的情况应在药物选择中发挥积极作用。应根据患者的身体和心理合并症、消化系统、药物敏感性、体重、睡眠、对药物反应的家族史、经济状况、是否有每日服用药物的意愿以及许多其他因素来选择预防类药剂。疲劳和/或体重增加是患者放弃预防类药剂的主要原因。头痛患者通常抱怨疲劳,并倾向于放弃增加疲劳的药物。患者的职业也可能引导护理人员放弃使用某些药物;例如,会计师可能无法忍受托吡酯带来的记忆问题。
Side effects are possible with any medication; the patient must be prepared to endure mild side effects in order to achieve results.
任何药物都有可能产生副作用;病人必须准备好忍受轻微的副作用,以达到效果。
First-line Preventive Medications for Migraine/偏头痛的一线预防性药物
Botulinum Toxin A/肉毒杆菌毒素A
Botulinum toxin A (Botox) has been studied extensively in patients with migraines. Nearly 8 million people have had botulinum toxin A injections for headache.⁴ Botulinum toxin A has been found to significantly improve quality of life and reduce headache impact. Botox is the only botulinum toxin A that is FDA-approved for treatment of chronic migraine. It is relatively safe and only takes a few minutes to inject. One set of injections may decrease headaches for 1 to 3 months. There also is a cumulative benefit, where the headaches continue to improve over 1 year of injections. Botox may be safer than many of the medications that are used for headache. Botox does not cause the “annoying” side effects that are commonly encountered with preventives. Except for the cost, the experience with Botox has been very positive.
肉毒杆菌毒素A(Botox)已经在偏头痛患者中进行了广泛的研究。近800万人因头痛而注射了A型肉毒杆菌毒素。肉毒杆菌毒素A已被发现可显著改善生活质量并减少头痛的影响。肉毒杆菌素是唯一经美国食品和药物管理局批准用于治疗慢性偏头痛的肉毒杆菌素A。它相对安全,只需要几分钟的注射时间。一组注射可以减少1至3个月的头痛。还有一种累积性的好处,即在注射1年后,头痛会继续改善。肉毒杆菌素可能比许多用于治疗头痛的药物更安全。肉毒杆菌毒素不会引起预防类药物通常带有的 "烦人"的副作用。除了费用之外,使用肉毒杆菌的经验结果是非常积极的。
Natural Supplements and Herbs/天然补充剂和草药
Feverfew, Petadolex (butterbur), and magnesium oxide have all proven effective in double-blind studies as migraine preventives. Of these, Petadolex has been the most effective.
小白菊、蜂斗菜根提取物(蜂斗)和氧化镁在双盲研究中均被证明是有效的偏头痛预防药物。其中,蜂斗菜根提取物是最有效的。
Petadolex is a purified form of the herb butterbur and is made of extracted plant certified by the German Health Authority. The herb preparation is commonly used in Europe, and has been found to be successful in preventing migraines in several well-designed blind studies. The usual dose is 100 mg per day, and many increase this to 150 mg daily (all at once, or in 2 divided doses). Earlier concerns about carcinogenesis with this family of herbs have decreased with the use of Petadolex. However, there are lingering concerns as to hepatotoxicity. Patients have occasionally experienced GI upset or a bad taste in the mouth, but Petadolex is usually well tolerated. It is prudent to stop it every six months or so.
蜂斗菜根提取物是一种蜂斗菜草药的纯化,由德国卫生局认证的提取植物制成。这种草药制剂在欧洲普遍使用,并在几项精心设计的盲法研究发现能够成功地预防偏头痛。通常的剂量是每天100mg,许多人将其增加到每天150mg(一次性服用,或分两次服用)。随着蜂斗菜根提取物使用,早先对这种草药家族的致癌性的担忧已经减少。但对肝脏毒性的担忧挥之不去。患者偶尔会出现肠胃不适或口中有异味,但蜂斗菜根提取物通常耐受性良好。谨慎的做法是每六个月左右停药一次。
Magnesium helps many systems in the body to function, especially the muscles and nerves. It has been shown that magnesium levels in the brains of migraine patients tend to be lower than normal. Magnesium oxide is used as a supplement to maintain adequate magnesium in the body. A dose of 400 or 500 mg per day can be used as a preventive; tablets are found in most pharmacies. However, mild GI side effects may limit use. There are also drug interactions that may occur; as always, consult your physician. There are tablets, as well as powdered versions available.
镁有助于身体的许多系统运作,特别是肌肉和神经。有研究表明,偏头痛患者大脑中的镁含量往往低于正常水平。氧化镁被用作补充剂以维持体内足够的镁。每天400或500mg的剂量可以作为预防类药剂;片剂在大多数药店都可以找到。然而,轻微的消化道副作用可能会限制其使用。还有可能发生药物相互作用;通常需要咨询主治医生。有片剂以及粉剂版本可供选择。
Feverfew has been demonstrated to be mildly effective in some patients for prevention of migraine headache. Feverfew can cause a mild increased tendency toward bleeding, and should be discontinued two weeks prior to any surgery. The problem with many herbal supplements is quality control. The amount of parthenolide (the active ingredient in feverfew) varies widely from farm to farm; certain farms consistently have better quality than others. The usual dose is 2 capsules each morning; there is a liquid form available. Patients occasionally will be allergic to feverfew, and it should not be used during pregnancy.
事实证明,小白菊对一些病人预防偏头痛有轻微的效果。小白菊可导致轻微出血倾向增加,因此应在任何手术前两周停药。许多草药补充剂的问题是质量控制。单叶菊内酯(小白菊中的活性成分)的含量因农场而异;某些农场的质量一直优于其他农场。通常的剂量是每天早上2粒;也有一种液体制剂可供选择。患者偶尔会对小白菊过敏,怀孕期间不应使用。
Miscellaneous herbs/supplements have been used, particularly vitamin B2. CoQ10 and fish oil have also been studied. These occasionally help, but are less effective than Petadolex. MigreLief has been a reliable combination of magnesium, riboflavin, and feverfew. The usual dose is 2 capsules per day, as a preventive. Most people order fromMigreLief.
已经使用了各种草药/补充剂,特别是维生素B2。辅酶Q10和鱼油也被研究过。这些偶尔会有帮助,但不如蜂斗菜根提取物有效。MigreLief是一种镁、核黄素和小白菊的有效组合。通常的剂量是每天2粒,作为一种预防性药物。大多数人直接从MigreLief订购。
Medications: First-line/药物:一线治疗
Topiramate is an effective migraine preventive, without the weight gain commonly encountered with the other meds. While usually fairly well tolerated, common side effects include memory difficulties (“spaciness”), and tingling. In higher doses, topiramate increases the risk for kidney stones. Topiramate does decrease appetite, leading to weight loss for some patients. This anorexic effect tends to disappear after several months. The usual dose is 50 mg to 100 mg daily, but some do well on as little as 25 mg. The dose may be pushed to 300 or 400 mg per day, in the absence of significant side effects. Topiramate is primarily used for migraine prevention, but has also been utilized for cluster and tension headache as well. Topiramate may cause a metabolic acidosis, with lower bicarbonate levels (and increased chloride). The acidosis may lead to the tingling, which sometimes is alleviated by increasing potassium-containing fruits/vegetables (or adding potassium). Trokendi XR is an excellent long-acting form of topiramate, approved for migraine prophylaxis. The FDA also approvedQudexy XR (topiramate) for once-daily dosing.
托吡酯是一种有效的偏头痛预防类药剂,不会出现其他药物常见的体重增加现象。虽然通常耐受性相当好,但常见的副作用包括记忆困难("空间感")和刺痛。高剂量时,托吡酯会增加肾结石的风险。托吡酯证实会降低食欲,导致一些病人体重下降。这种厌食效应通常在几个月后会消失。一般剂量是每天50mg至100mg,但有些人剂量在25mg时效果也很好。在没有明显副作用的情况下,剂量可推至每天300或400mg。托吡酯主要用于预防偏头痛,但也被用于治疗丛集性和紧张性头痛。托吡酯可能引起代谢性酸中毒,伴有碳酸氢盐水平降低(而氯化物增加)。这种酸中毒可能导致刺痛,有时通过增加含钾的水果/蔬菜(或增加钾)可以缓解刺痛。Trokendi XR是一种极好的长效型托吡酯,被批准用于偏头痛的预防。FDA还批准了Qudexy XR(托吡酯)每日一次的剂量。
Valproate, or divalproex sodium (Depakote), is a longtime staple, popular for migraine prevention. It is usually well tolerated in the lower doses used for headaches; however, the generic may not be as effective. Liver functions need to be monitored in the beginning of treatment. Valproate also is one of the primary mood stabilizers for bipolar disorder. Oral Depakote ER (500 mg) is an excellent once-daily, long-acting agent. As with most preventives, valproate needs 4 to 6 weeks to become effective.
丙戊酸盐或二丙戊酸钠(Depakote)是一种长期使用的主要药物,常用于预防偏头痛。在用于治疗头痛的较低剂量下,通常具有良好的耐受性;但是,仿制药可能不那么有效。在治疗开始时需要监测肝功能。丙戊酸盐也是双相情感障碍的主要情绪稳定剂之一。口服Depakote ER(500mg)是一种很好的每日一次的长效药物。与大多数预防类药剂一样,丙戊酸盐需要4至6周才能生效。
The β-blocker propranolol also is FDA approved as a preventive agent for migraines. Long-acting oral propranolol (Inderal), for example, is very useful in combination with the tricyclic antidepressant amitriptyline. Dosage begins with the long-acting agent given at 60 mg per day, and is usually kept between 60 and 120 mg per day. Lower doses are sometimes effective, such as 20 mg twice a day of propranolol. Other β-blockers also are effective, such as metoprolol (Toprol XL) and atenolol. Some of these are easier to work with than propranolol because they are scored tablets, and metoprolol and atenolol have fewer respiratory effects. Depression may occur. β-blockers are useful for those migraine patients with concurrent hypertension, tachycardia, mitral valve prolapse, and panic/anxiety disorders. Bystolic (nebivolol) is another β-blocker that may be helpful for the prevention of headaches, and has fewer respiratory side effects than other agents. Bystolic probably has the fewest side effects among the β-blockers.
β-受体阻滞剂普萘洛尔也被FDA批准作为偏头痛的预防类药剂。例如,长效口服普萘洛尔(Inderal)与三环类抗抑郁药阿米替林联合使用非常有效。剂量从长效制剂开始,每天60mg,通常保持在每天60至120mg之间。较低的剂量有时也有效,如普萘洛尔20mg,每天两次。其他β-受体阻滞剂也是有效的,如美托洛尔(Toprol XL)和阿替洛尔。其中一些比普萘洛尔更容易操作,因为它们是切分药片,而且美托洛尔和阿替洛尔对呼吸系统的影响更小。可能会出现抑郁症。β-受体阻滞剂对那些并发高血压、心动过速、二尖瓣脱垂和惊恐/焦虑症的偏头痛患者很有用。Bystolic(nebivolol)是另一种β-受体阻滞剂,可能对预防头痛有帮助,而且比其他药物有较少的呼吸系统副作用。在β-受体阻滞剂中,Bystolic的副作用可能是最小的。
As noted, amitriptyline is an effective, inexpensive agent that is useful for the prevention of daily headaches and insomnia. As a preventive agent, amitriptyline is prescribed at low doses and taken at night. Sedation, weight gain, dry mouth, and constipation are common side effects. Other tricyclic antidepressants such as doxepin and protriptyline can be effective for migraine. Nortriptyline is similar to amitriptyline, with somewhat fewer side effects. These also are used for daily tension-type headaches. Protriptyline is one of the few older antidepressants that does not cause weight gain. However, anticholinergic side effects are increased with protriptyline; protriptyline is more effective for tension headache than for migraine. Although selective serotonin reuptake inhibitors (SSRIs) are used, they are more effective for anxiety and depression than for migraine.
如前所述,阿米替林是一种有效的、廉价的药剂,可用于预防日常头痛和失眠。作为一种预防类药剂,阿米替林的剂量很低,在晚上服用。镇静、体重增加、口干和便秘是常见的副作用。其他三环类抗抑郁药,如多塞平和普瑞替林对偏头痛也有疗效。去甲替林与阿米替林相似,副作用稍小。这些药物也用于治疗日常紧张型头痛。普瑞替林是少数不会导致体重增加的老牌抗抑郁药之一。然而,抗胆碱能的副作用会因丙戊酸钠而增加;丙戊酸钠对紧张性头痛比对偏头痛更有效。虽然有人使用选择性5-羟色胺再摄取抑制剂(SSRIs),但它们对焦虑和抑郁症比对偏头痛更有效。
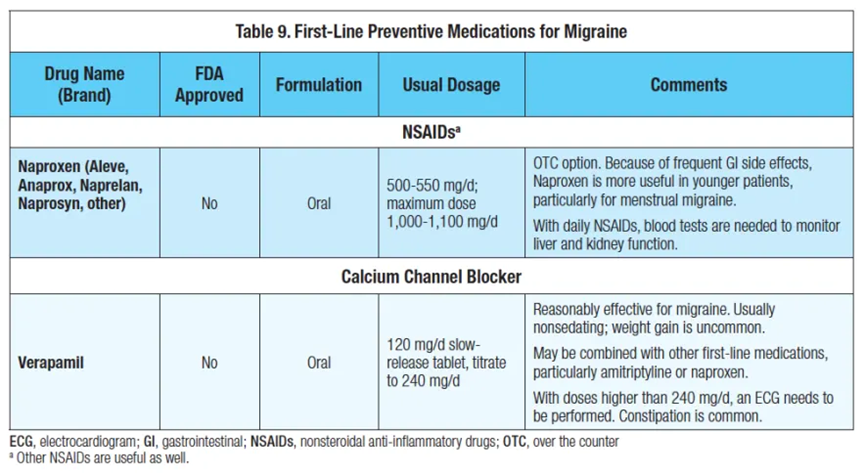
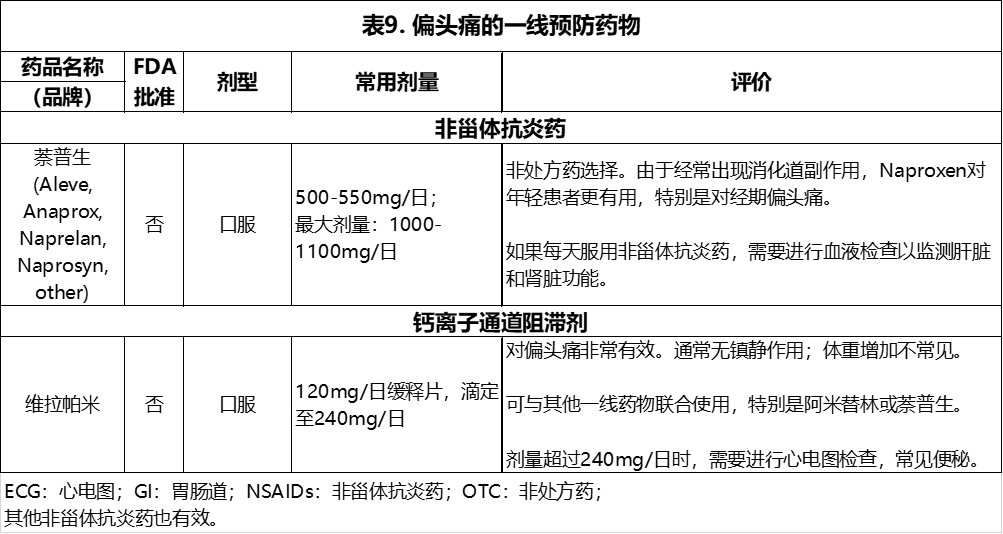
Naproxen is a very useful agent for the treatment of daily headaches, as well as for younger women suffering from menstrual migraine. Naproxen is nonsedating, but frequently causes GI upset or pain. Effective as an abortive, it may be combined with other first-line preventive medications. Other NSAIDs can similarly be used for migraine prevention. It is crucial to use low doses. As with all anti-inflammatories, GI side effects increase as people age, and therefore NSAIDs are used more often in the younger population. Blood tests are needed to monitor liver and kidney function.
萘普生是一种非常有用的治疗日常头痛的药物,也是治疗年轻女性经期偏头痛的药物。萘普生不具有镇静作用,但经常引起消化道不适或疼痛。作为一种有效的中止剂,它可以与其他一线预防药物结合使用。其他非甾体抗炎药也同样可用于预防偏头痛。使用小剂量是关键。与所有消炎药一样,消化道副作用随着人们年龄的增长而增加,因此非甾体抗炎药在年轻人群中更常用。需要进行血液检查以监测肝脏和肾脏功能。
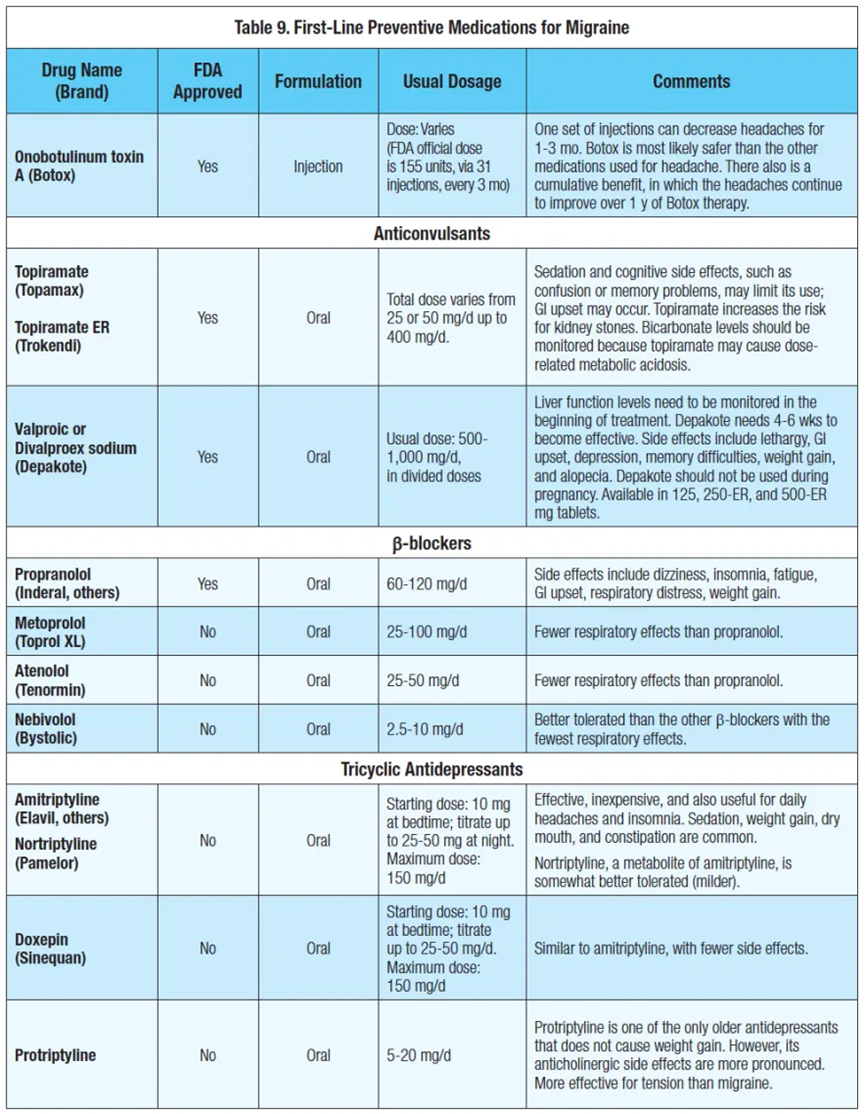
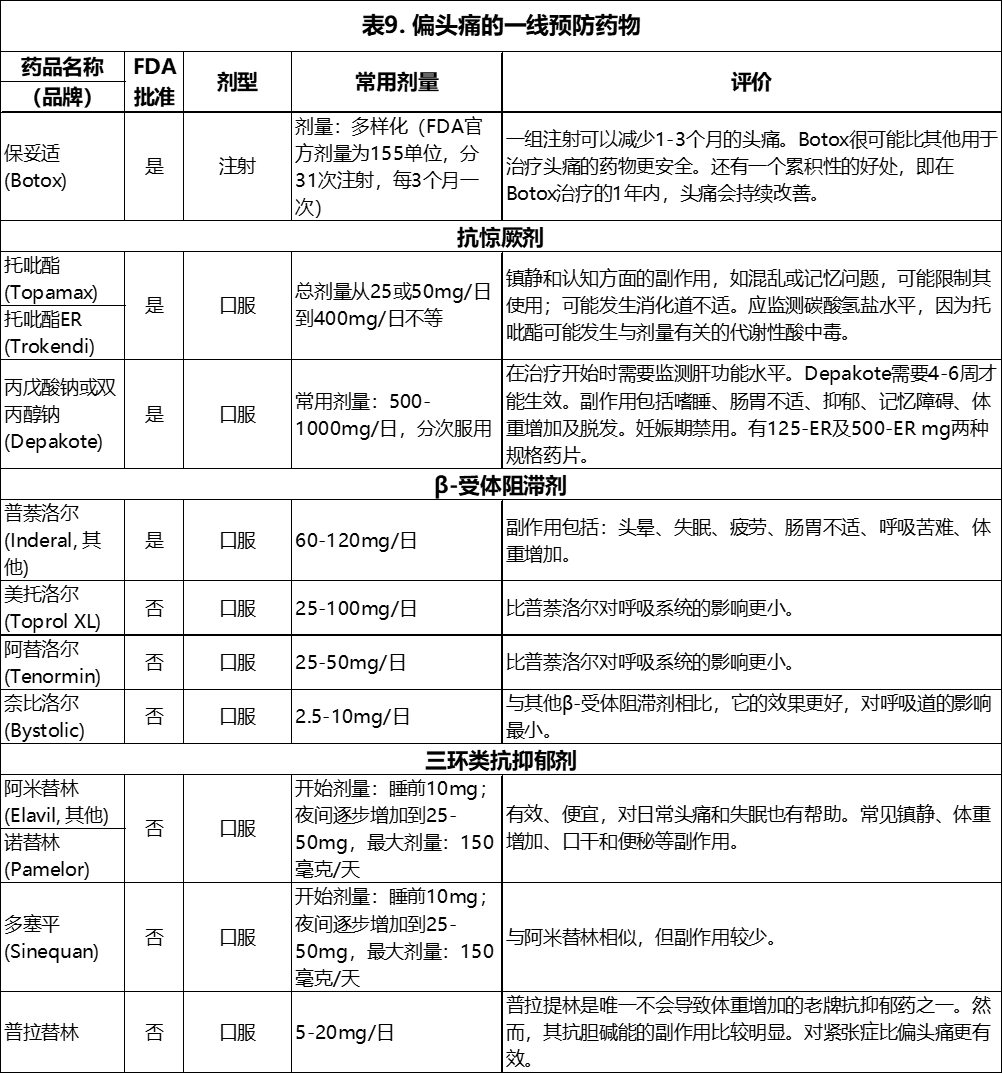
Table 9 reviews first-line migraine preventive therapy.
表9综述了一线偏头痛预防疗法。
接下文Part.2
- 还没有人评论,欢迎说说您的想法!