

译作分享
译者:李昭兴
Migraine is a very common and disabling illness. Picking an agent that is best for each individual patient requires considering the patient’s history, lifestyle, comorbid conditions, and individual preferences. There are a few new treatment options, including TMS and ketamine.
偏头痛是一种非常常见的致残疾病。为每位患者选择最适合的药物需要考虑患者的病史、生活方式、合并症情况及个体偏好。目前有一些新的治疗方案,包括经颅磁刺激和氯胺酮。
CITE THIS ARTICLE/引用此文
Robbins L. Migraine Treatment: What’s Old, What’s New. Pract Pain Manag. 2017;17(5).
Migraine headaches are a common cause of disability in the United States, affecting approximately 27 million American adults, or 17.1% of women and 5.6% of men.¹ To help better define migraines, the term classical migraine has been replaced with migraine with aura, and non-classical migraine is now referred to as migraine without aura. Chronic migraine, which affects 3.2 million Americans (2%), is defined as having migraine symptoms for at least 15 days per month, lasting at least 4 hours, and for longer than 3 months in duration. This is in contrast to episodic migraine, which causes symptoms on fewer than 15 days per month.² Current treatment for chronic migraine is divided into acute, abortive agents (analgesics, triptans, ergots, etc.), and medications that will prevent migraine onset.
偏头痛是美国人致残的一个常见原因,影响了大约2700万美国成年人,即17.1%的女性和5.6%的男性¹。为了帮助更好地定义偏头痛,“传统偏头痛”一词已被“有先兆的偏头痛”所取代,而“非传统偏头痛”现在被称为“无先兆偏头痛”。影响320万美国人(2%)的每月至少有15天出现偏头痛症状,持续时间至少4小时,并且持续时间超过3个月,被定义为慢性偏头痛。这与每月出现症状少于15天的发作性偏头痛形成鲜明对比²。目前对慢性偏头痛的治疗分为急性、中止性药物(镇痛剂、三苯氧胺、麦角类药物等)和防止偏头痛发作的药物。
This review will highlight the current definitions of migraines as well as treatment options.
本综述将强调目前对偏头痛的定义以及治疗方案。
Migraine Characteristics/偏头痛的特点
A recurring headache that is of moderate or severe intensity, and is triggered by migraine-precipitating factors, usually is considered to be migraine. Precipitating factors can include stress, certain foods, weather changes, smoke, hunger, fatigue, hormones, and so on. Migraine without aura is a chronic idiopathic headache disorder with attacks lasting 4 to 72 hours. Status migrainosus applies to migraine headaches that exceed 72 hours. Migraine features often include a unilateral location and a throbbing or pulsating nature to the pain. There may be associated nausea, photophobia, phonophobia, or dizziness (Table 1). Further characteristics include a positive relationship with menses, decreased frequency during pregnancy, increased pain with physical activity, and history of migraine in first-degree relatives. It has been reported by 70% to 75% of migraine patients that they have a first-degree relative with a history of migraines.³
中度或重度反复发作的头痛,如果是由偏头痛的诱发因素引发的,通常被认为是偏头痛。诱发因素可以包括压力、某些食物、天气变化、烟雾、饥饿、疲劳、荷尔蒙,等等。无先兆偏头痛是一种慢性特发性头痛疾病,发作持续4至72小时。超过72小时的偏头痛称为偏头痛持续状态。偏头痛的特征通常包括单侧位置跳动或脉动性疼痛。可能伴有恶心、畏光、畏声或头晕(表1)。其他特征包括与月经期呈正相关,怀孕期间频率降低,体力活动时疼痛加剧,以及一级亲属有偏头痛史。据报道,70%至75%偏头痛患者有一级亲属偏头痛病史³。
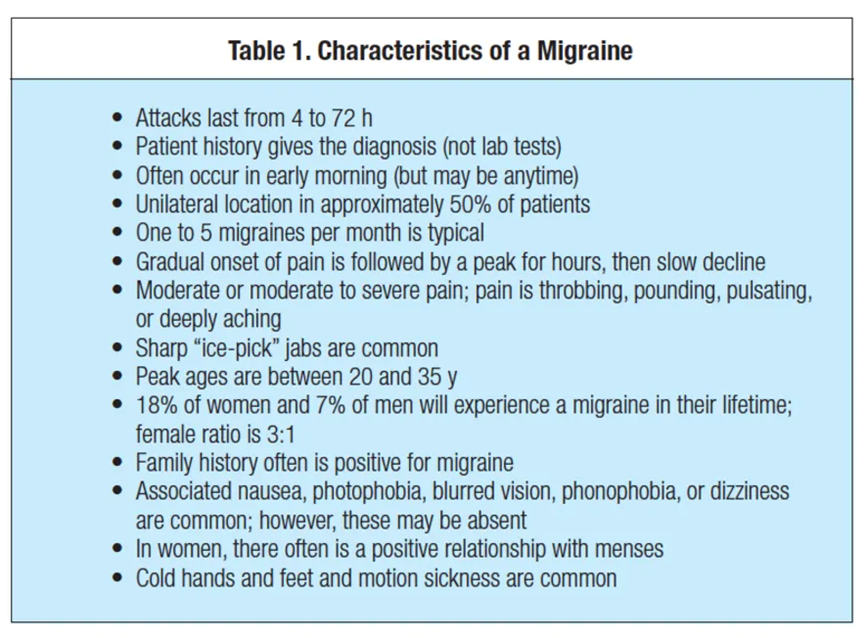
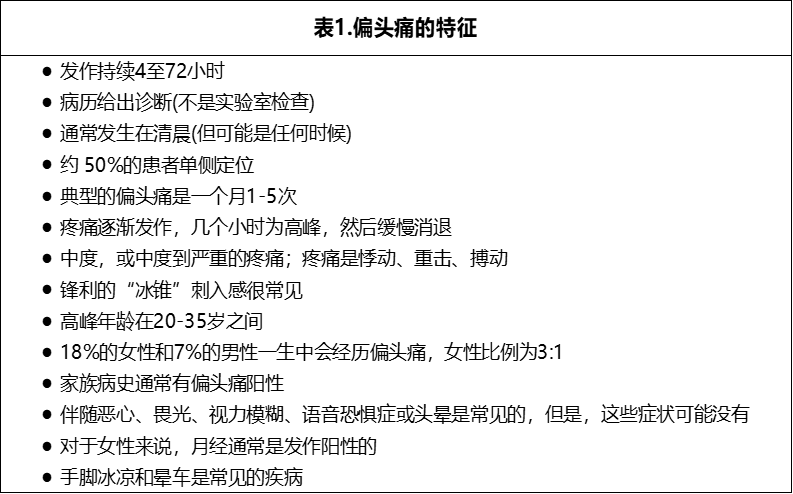
Patients who suffer from migraines often have colder hands and feet compared with controls, and the prevalence of motion sickness is much higher in migraine patients. Although most patients will not have all of these characteristics, there are certain diagnostic criteria that have been established by the International Headache Society for the definite diagnosis of migraine.² Distinguishing a milder migraine without aura from a moderate or severe tension headache may be difficult, and it is not surprising when “pure” migraine medications are effective for severe tension-type headaches.
与对照组相比,偏头痛患者的手脚往往更冷,而且偏头痛患者晕车的发生率要高得多。尽管大多数患者不会具备所有这些特征,但国际头痛协会已经制定了一定的诊断标准,可以明确偏头痛的诊断²。区分较轻度无先兆偏头痛和中度或重度紧张性头痛可能很困难,因此当 "纯 "偏头痛药物对重度紧张型偏头痛有效时,也就不足为奇了。
Recurrent, repeated attacks of throbbing or severely aching headache are generally regarded as migraine, whether or not the patient has nausea, dizziness, photophobia, or phonophobia. The patient’s history is used to make the diagnosis of migraine. Physical examination and magnetic resonance imaging (MRI) or computed tomography (CT) scans are helpful only in ruling out organic pathology. Recent-onset headaches need to be investigated with an MRI to rule out other organic disorders, particularly brain tumors. In addition to physical exam and imaging, a check of intraocular pressure (IOP) may be warranted. With new-onset headaches, an eye exam is always warranted.
复发性、反复发作的搏动性或严重疼痛的头痛一般被认为是偏头痛,无论病人是否有恶心、头晕、畏光或畏音的症状。患者的病史可用于诊断偏头痛。身体检查和磁共振成像(MRI)或计算机断层扫描(CT)仅有助于排除器质性病变。近期发作的头痛需要用核磁共振成像进行检查,以排除其他器质性疾病,特别是脑肿瘤。除了体格检查和影像学检查外,可能还需要检查眼压(IOP)。对于初发病的头痛,一般进行眼部检查是必要的。
Although the pain is unilateral in 50% of migraine patients, the entire head often becomes involved. The pain may be in the facial or the cervical (neck) areas, and often will shift sides from one occurrence to another. Most patients, however, suffer the severe pain on one favored side from attack to attack.
虽然50%的偏头痛患者的疼痛是单侧的,但通常会累及整个头部。疼痛可能发生在面部或颈部,经常会从一个部位转移到另一个部位。然而,大多数病人在一次又一次的发作中,只承受偏向一侧的剧烈疼痛。
The typical migraine patient suffers 1 to 5 attacks in a month, but many patients average l<1 (episodic) or >10 per month (chronic). The attack frequency varies with the seasons, and many patients can identify a time of year when their headaches increase significantly. Patients with chronic migraine may have 15 days a month of headache, and many even have 30 days/month, 24/7.
典型的偏头痛患者在一个月内遭受 1 至 5 次发作,但许多患者平均每月 l<1(发作性)或 >10(慢性)。发作频率随季节而变化,许多患者可以确定一年中头痛明显加重的时间。慢性偏头痛患者可能每月头痛15天,许多人甚至有30天/月、24小时不间断的头痛。
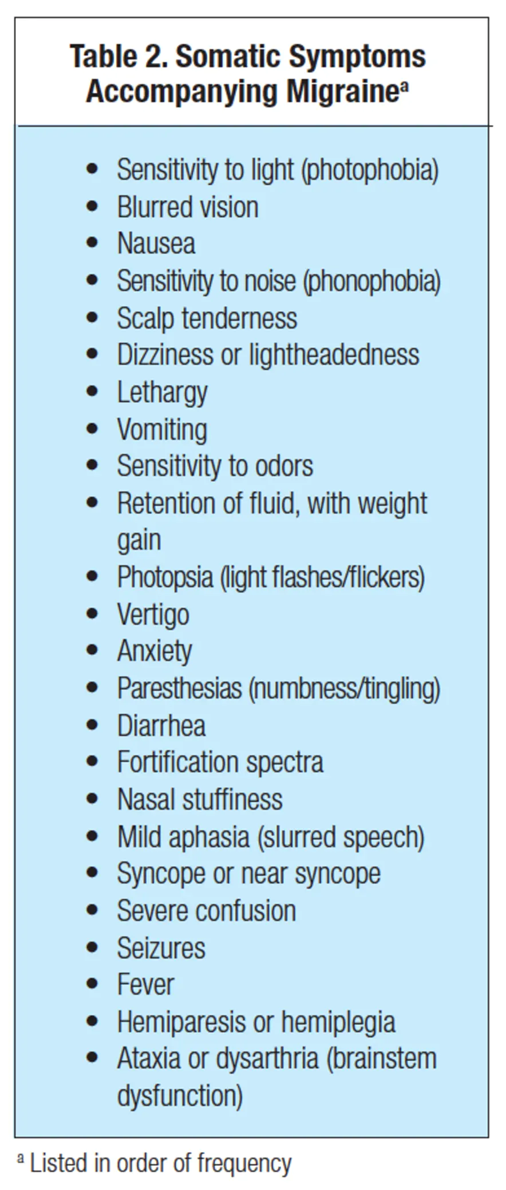
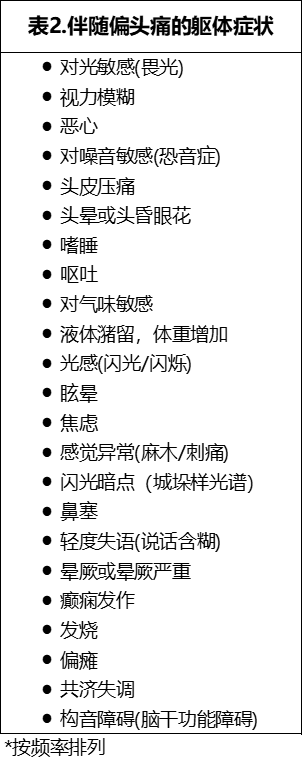
The pain of a migraine often follows a bell-shaped curve, with a gradual ascent, a peak for a number of hours, and then a slow decline (Table 2). Occasionally, the pain may be at its peak within minutes of onset. Many patients with migraine suffer some degree of nausea during the attack, and some experience vomiting as well. The nausea often is mild, and some patients are not bothered by it. Many patients state that the headache is lessened after they vomit. Diarrhea may occur and is usually mild to moderate. The presence of diarrhea renders the use of rectal suppositories impossible.
偏头痛的疼痛通常遵循钟形曲线,逐渐上升,数小时内达到峰值,然后缓慢下降(表2)。有时,疼痛可能在发病后几分钟内达到高峰。许多偏头痛患者在发作期间遭受一定程度的恶心,有些人也会呕吐。恶心通常是轻微的,有些患者并无恶心症状。许多患者表示,呕吐后头痛减轻。可能发生腹泻,通常为轻度至中度。腹泻时不得使用直肠栓剂。
Lightheadedness often accompanies the migraine, and syncope may occur. Most patients become sensitive to bright lights, sounds, and/or odors. Between migraine attacks, many patients retain the photophobia, and it is common for migraine patients to wear sunglasses most of the time. Sensitivity to bright lights is a distinctive migraine characteristic.
偏头痛常伴有头晕,也可能发生晕厥。大多数病人对强光、声音和/或气味敏感。在偏头痛发作期间,许多患者仍有畏光症,且偏头痛患者大部分时间都戴太阳镜是很常见的。对强光敏感是偏头痛的一个明显特征。
Pallor of the face is common during a migraine; flushing may occur as well but is seen less often. Patients do complain of feeling excessively hot or cold during an attack, and the skin temperature may increase or decrease on the side with pain. Patients with migraines often experience tenderness of the scalp that may linger for hours or days after the migraine pain has ceased. This tenderness may actually occur during the prodrome of the migraine. Both vascular and muscular factors contribute to the scalp tenderness. Autonomic disturbances are relatively common, such as pupillary miosis or dilation, rhinorrhea, eye tearing, and nasal stuffiness. These also are symptoms of cluster headache, including the sharp pain around one eye or temple.
偏头痛期间面色苍白很常见;也可能出现面色潮红,但较少见。有患者抱怨在发作期间感觉过热或过冷,有疼痛的一侧皮肤温度可能会升高或降低。偏头痛患者经常会出现头皮压痛,在偏头痛停止后头皮压痛可能会持续数小时或数天。这种压痛实际上可能发生在偏头痛的前驱期。血管和肌肉因素都会导致头皮压痛。自主神经紊乱相对常见,例如瞳孔瞳孔缩小或扩张、流涕、眼撕裂和鼻塞。这些也是丛集性头痛的症状,包括一只眼睛或太阳穴周围的剧烈疼痛。
Alterations of mood are seen with many patients before, during, and after migraine attacks. Patients are usually anxious, tired, or depressed. They often feel “washed out” after an attack, but a calm or even euphoric state occasionally is seen as a postdrome to the migraine. Rarely, euphoria or exhilaration may precede a migraine.
许多患者在偏头痛发作之前、期间和之后都会出现情绪变化。患者通常会感到焦虑、疲惫或抑郁,经常在偏头痛发作后感到“精疲力竭”,但平静甚至欣快的状态偶尔也被视为偏头痛的后期。极少数情况下偏头痛发作前会出现欣快或兴奋。
Weight gain due to fluid retention may occur, and begins prior to the onset of a migraine. At some point during the migraine, patients may experience polyuria. The weight gain is usually less than 4 lb, and is transient.
可能会出现因液体潴留而导致的体重增加,并在偏头痛发作前开始。在偏头痛发作期间,患者可能会出现多尿。体重增加通常不超过4磅,且是暂时性的。
Visual Disturbances/视觉障碍
Approximately 20% of patients experience visual neurologic disturbances preceding or during the migraine; these auras may be as disturbing to the patient as the migraine pain itself. The visual symptoms usually last 15 to 20 minutes, and most often will be followed by the migraine. Most migraine sufferers experience the same aura with each migraine, but occasionally one person may have several types of auras. “The light of a flashbulb going off” is the description many patients give to describe their aura. The visual hallucinations reported most often consist of spots, stars, lines (often wavy), color splashes, and waves resembling heat waves. The images may seem to shimmer, sparkle, or flicker. These visual occurrences are referred to as photopsia.
大约20%的患者在偏头痛发作前或发作期间会出现视觉神经障碍;这些先兆对患者来说可能和偏头痛本身一样令人不安。视觉症状通常持续15到20分钟,最常见的是随之出现的偏头痛。大多数偏头痛患者每次偏头痛都有相同的先兆,但偶尔有人可能有几种先兆。“闪光灯一闪而过”是许多患者对先兆的描述。据描述,视觉幻觉通常包括斑点、星星、线条(通常是波浪状)、颜色飞溅和类似热浪的波浪。图像看起来可能是闪闪发光、星点光或闪烁的。这些视觉现象被称为“光幻视”。
Fortification spectra are seen much less often than photopsia. They usually begin with a decrease in vision and visual hallucinations that are unformed. Within minutes, a paracentral scotoma becomes evident and assumes a crescent shape, usually with zigzags. There often is associated shimmering, sparkling, or flickering at the edges of the scotoma.
强化光谱比畏光更少见。通常以视力下降和未形成的视觉幻觉开始。在几分钟内,中心旁暗点变得明显并呈现新月形,通常还有之字形。暗点的边缘常伴有微光、闪光或闪烁。
Patients may experience a “graying out” of their vision, or a “white out” may occur. Some patients suffer complete visual loss, usually for some minutes. Photopsia may be experienced at the same time as the gray-out, white- out, or visual loss.
患者可能会经历视力“变灰”,或可能发生“白化”。一些患者遭受完全的视力丧失,通常持续几分钟。光幻觉可能与灰显、白化或视力丧失同时出现。
Miscellaneous Neurologic Symptoms/其他神经系统症状
Numbness or tingling (paresthesias) commonly are experienced by patients as part of the migraine. These are experienced most often in one hand and forearm, but may be felt in the face, peri-orally, or in both arms and legs. Like the visual disturbances, they often last only minutes preceding the pain, but the numbness may continue for hours, and at times the paresthesias are severe. The sensory disturbances usually increase slowly over 15 to 25 minutes, differentiating them from the more rapid pace seen in epilepsy.
作为偏头痛的一部分,患者通常会有麻木或刺痛(Paresthesias)的感觉。这些症状最常出现在一只手和前臂,但也可能出现在面部、口周或双臂和双腿。与视觉障碍一样,它们往往在疼痛之前只持续几分钟,但麻木感可能持续数小时,有时麻痹感会很严重。感觉障碍通常在15至25分钟内缓慢增加,将其与癫痫中较快的麻痹速度区分开来。
Paralysis of the limbs may occur, but this is rare. This is occasionally seen as a familial autosomal dominant trait, and the term familial hemiplegic migraine is applied to this form. With the weakness, aphasia or slurred speech may also occur, and sensory disturbances are seen ipsilateral to the weakness.
也可能会发生肢体瘫痪,但这是罕见的。这种情况偶尔见于家族性常染色体显性遗传,这种病症的术语称为家族性偏瘫性偏头痛。随着身体的虚弱,还可能出现失语症或言语不清,感觉障碍见于虚弱的同侧。
Vertigo and/or dizziness are often experienced during migraine, and may be disabling. “Migraine associated vertigo” has become a common diagnosis. At times, the dizziness is more disabling to patients than the other symptoms. Ataxia may occur, but is not common. Rarely, multiple symptoms of brain stem dysfunction occur, with the term basilar migraine being applied to this type of syndrome. The attack usually begins with visual disturbances (most often photopsia), followed by ataxia, vertigo, paresthesias, and other brain stem symptoms. These severe neurologic symptoms usually abate after 15 to 30 minutes, and are followed by a headache. This type of migraine often stops over months or years, and the patient is simply left with migraine headaches without neurologic dysfunction.
眩晕和/或头晕在偏头痛期间经常出现,并可能造成残疾。"偏头痛相关眩晕 "已成为一种常见的诊断。有时,头晕比其他症状更能使患者丧失能力。共济失调可能发生,但并不常见。极少数情况下,会出现多种脑干功能障碍的症状,这种类型的综合征术语称为基底偏头痛。发作时通常以视觉障碍(最常见的是畏光)开始,随后是共济失调、眩晕、麻痹和其他脑干症状。这些严重的神经系统症状通常在15至30分钟后减轻,随后是头痛。这种类型的偏头痛常常在几个月或几年后停止,病人通常仍患有偏头痛,但不再有神经系统功能障碍。
Workup for Migraine/偏头痛的病情检查
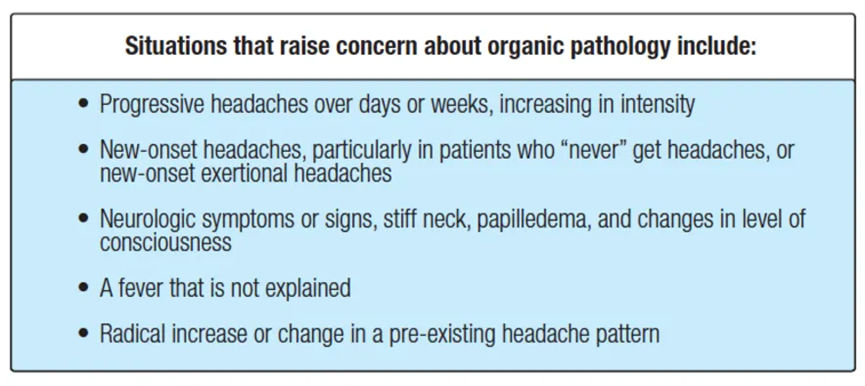
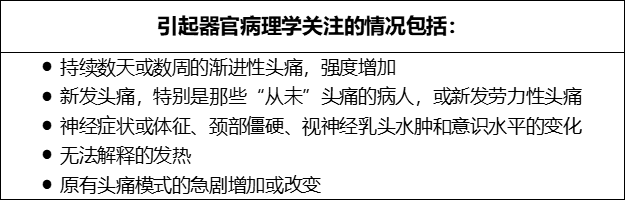
As noted, when patients present with a long history of typical migraine attacks, and the headaches are essentially unchanged, scans of the head usually are not absolutely necessary. Whether to do any testing at all depends on the physician’s clinical suspicion of organic pathology (see box). Sound clinical judgment, based on patient history and a physical exam, is crucial in deciding who needs which exam.
如前所述,当患者长期存在典型的偏头痛发作史,并且头痛基本没有变化时,头部扫描通常不是绝对必要的。是否采取任何检查取决于医生对器质性病理的临床怀疑(见方框)。基于患者病史和体格检查,合理的临床判断对于决定个性化检查至关重要。
In addition to the MRI and CT scan, tests that are sometimes useful for diagnosis of headache, include lumbar puncture, IOP testing, CT scan of the sinuses, and blood tests. A magnetic resonance angiogram (MRA) allows the detection of most intracranial aneurysms.
除了核磁共振成像和CT扫描外,还有一些测试有时也对头痛的诊断有用,包括腰椎穿刺、眼压测试、鼻窦CT扫描和血液检查。磁共振血管造影(MRA)可以检测出大多数颅内动脉瘤。
The problems that need to be excluded in a patient with new-onset migraine include sinus disease, meningitis, glaucoma, brain tumor, arteritis, subarachnoid hemorrhage, low pressure headache, idiopathic intracranial hypertension, hydrocephalus, pheochromocytoma, stroke or transient ischemic attack, internal carotid artery dissection, and systemic illness.
初发病的偏头痛患者需要排除的问题包括窦性疾病、脑膜炎、青光眼、脑肿瘤、动脉炎、蛛网膜下腔出血、低压头痛、特发性颅内高压、脑积水、嗜铬细胞瘤、卒中或短暂性脑缺血发作、颈内动脉夹层和全身性疾病。
Headache Triggers/头痛诱因
With migraine and chronic daily headache sufferers, avoidance of triggers should be emphasized. The most common triggers are stress (both during and after stress), weather changes, perimenstruation, missing meals, bright lights or sunlight, under- and oversleeping, food sensitivity, perfume, cigarette smoke, exercise, and sexual activity. Some foods can be headache triggers, but foods tend to be overemphasized. In general, headache patients do better with regular schedules, eating three or more meals per day and going to bed and waking at the same time every day. Many patients state that “I can tell the weather with my head.” Barometric changes and storms are typical weather culprits, but some patients do poorly on bright “sun-glare” days.
对于偏头痛和慢性日常头痛患者,应强调避免触发诱因。最常见的诱因是压力(包括压力期间和之后)、天气变化、月经期、缺餐、强光或阳光、睡眠不足或睡眠时间过长、食物敏感、香水、香烟烟雾、运动和性行为。有些食物可能会引发头痛,但食物往往被过度强调。一般来说,有规律的作息,每天三餐或多餐,每天在同一时间睡觉和起床,头痛患者的表现会更好。许多病人说:“我可以用我的头判断天气。”气压变化和风暴是典型的诱因,但有些病人在明亮的“阳光灿烂”的日子里表现不佳。
Regarding stress as a trigger, it is not so much extreme stress, but daily hassles that increase headaches. When patients are faced with overwhelming daily stress, particularly when they are not sleeping well at night, headaches can be much worse the next day.
关于压力是一个诱因,与其说是极端的压力造成头痛,不如说是日常的困扰增加了头痛。当病人面临压倒性的日常压力时,特别是当他们晚上睡不好的时候,第二天头痛会更严重。
Psychotherapy is extremely useful for many headache patients with regard to stress management, coping, life issues, family-of-origin issues, and so on. Although psychotherapy may be recommended, it is crucial to legitimize the headaches as a physical condition; headaches are not a “psychological” problem, but rather a physical one that stress may exacerbate. Once one inherits the brain chemistry for headache, these triggers come into play; without the inherited genetics, most people may have stress/weather changes/hormonal changes, but not experience a headache.
心理治疗对于许多头痛患者在压力管理、应对生活问题、家庭问题等方面非常有用。尽管可以推荐进行心理治疗,但将头痛正视为一种身体状况至关重要;头痛不是“心理”问题,而是因压力可能加剧的身体问题。一旦有人遗传了头痛的大脑化学反应,这些触发因素就会发挥作用;如果没有遗传基因,大多数人可能会有压力/天气变化/荷尔蒙变化,但不会感到头痛。
Managing stress with exercise, yoga/Pilates/meditation, etc., often will reduce the frequency of headaches. The ideal would be for the patient to take a class weekly, then do the stretches and breathing for 10 minutes a day. Patients may experience some relief from associated neck or back pain. Relaxation techniques such as biofeedback, deep breathing, and imaging also may be helpful for daily headache patients, particularly when stress is a factor.
通过运动,瑜伽/普拉提/冥想等方式管理压力,通常会减少头痛的频率。理想情况是患者每周上一堂课,然后每天做10分钟伸展运动和深呼吸。患者可能会减轻相关的颈部或背部疼痛。诸如生物反馈训练、深呼吸和冥想等放松技巧也可能对日常头痛患者有帮助,特别是当压力为其中一个诱因时。
Many migraine patients have accompanying neck pain and physical therapy may help; acupuncture or chiropractic treatments occasionally help. Certain physical therapists “specialize” in head and neck pain. Massage may be effective, but the relief is often short-lived. Temporomandibular disorder (TMD), with clenching and/or bruxing, may exacerbate migraine; with TMD, physical therapy, a bite splint, and/or Botox may help. It often “takes a village” to help a person with pain, and we recruit other “villagers”, such as physical therapists or psychotherapists.
许多偏头痛患者伴有颈部疼痛,使用物理治疗可能会有所帮助;针灸或脊椎按摩偶尔有帮助。某些物理治疗师“专攻”头部和颈部疼痛。按摩可能是有效的,但缓解往往是短暂的。颞下颌紊乱(TMD)伴紧绷和/或磨擦,可加重偏头痛;对于TMD,物理治疗、夹板和/或肉毒杆菌可能会有所帮助。帮助一个有痛苦的人通常需要“全村的力量”,我们会招募其他“村民”,如物理治疗师或心理治疗师来帮助他。
Caffeine Use/咖啡因的使用
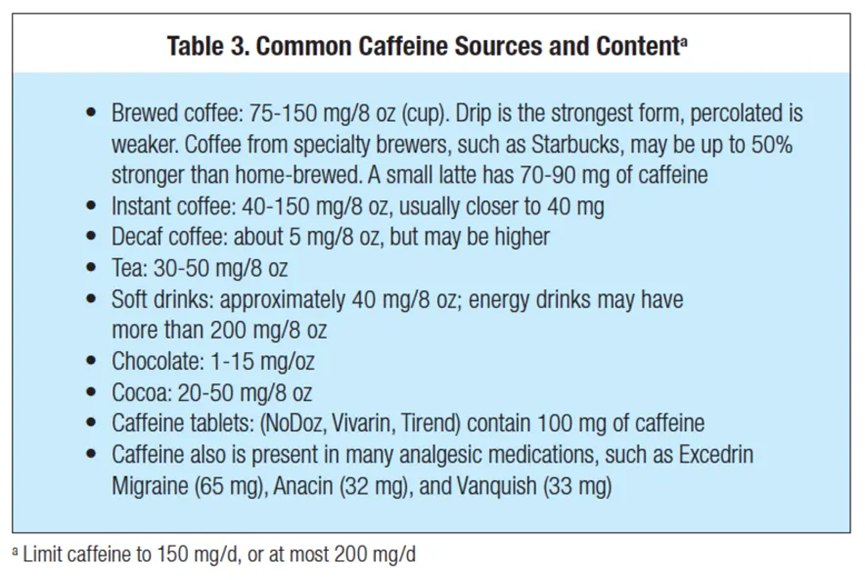
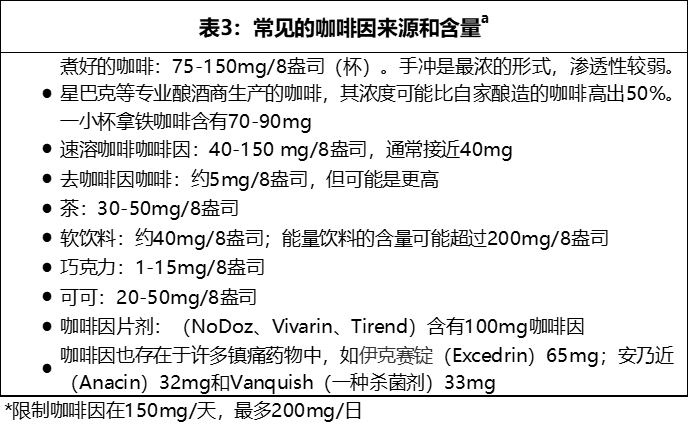
Although caffeine can help headaches, overuse may increase headaches. Whether in coffee, caffeine pills, or combination analgesics, patients must limit total caffeine intake. The maximum amount of caffeine taken each day varies from person to person, depending on sleep patterns, presence of anxiety, and sensitivity to possible rebound headaches. In general, caffeine should be limited to no more than 150 or 200 mg a day (Table 3).
尽管咖啡因对头痛有帮助,但过度使用可能会增加头痛。无论是咖啡、咖啡因药片,还是复合镇痛剂,患者必须限制咖啡因的总摄入量。每天摄入的最大咖啡因量因人而异,取决于睡眠模式、是否存在焦虑以及对可能的反跳性头痛的敏感性。一般来说,咖啡因应该限制在每天不超过150或200mg(表3)。
接下文Part.2
- 还没有人评论,欢迎说说您的想法!